Capsule diversity and epidemiology among K. pneumoniae causing newborn sepsis
Each year 100,000 newborns die from severe blood infections caused by the bacterium Klebsiella pneumoniae. The vast majority of infections are resistant to multiple antibiotics and occur in resource-limited settings, making them particularly difficult to treat.
There is an urgent need for new strategies to prevent newborn sepsis, and growing interest in a maternal vaccine targeting the K. pneumoniae polysaccharide capsule. But there are more than 160 different capsule types and only 15-20 can be included in a vaccine, so how do we know which ones to pick?
First, we need to understand which capsules are the most common causes of infections in high burden settings.
In our recent PLoS Medicine paper, we investigated genome-predicted capsule epidemiology among ~2000 K. pneumoniae causing newborn sepsis at 35 sites across Africa and Southern Asia. We used our genomic typing tool, Kaptive, to identify capsule loci (the genes encoding the capsules, also known as ‘K loci’), and applied Bayesian statistical models to estimate the frequencies of each locus in each of four key sub-continental regions and globally.
We found that the top 5 capsule loci together account for ~50% of all K. pneumoniae newborn sepsis cases globally and each was common in all geographic regions. A combination of 20 capsule loci accounted for >70% infections- the minimum coverage target for a vaccine- but geographic variation needs to be considered carefully to achieve the target for all regions.
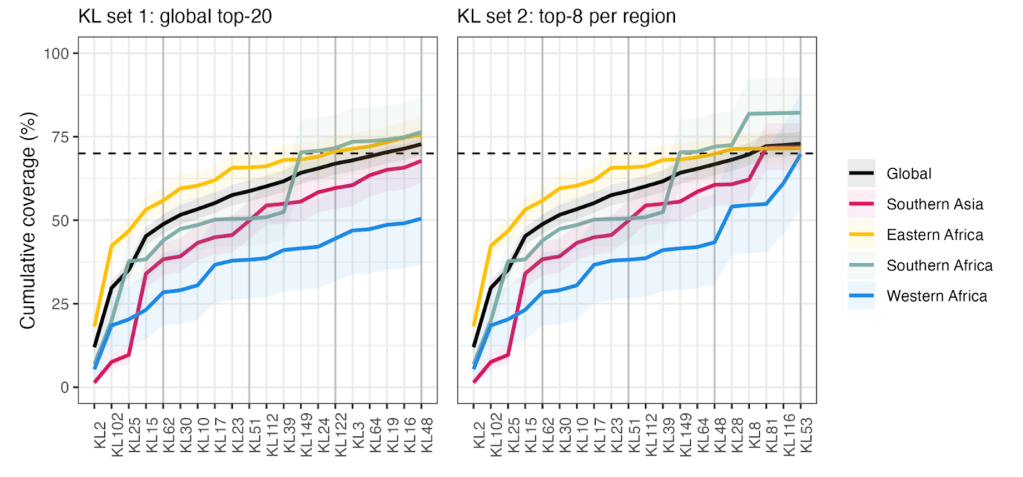
Figure caption: Theoretical population coverage of an anti-K. pneumoniae vaccine targeting 20 capsule types. Each panel shows the cumulative proportion of newborn sepsis isolates represented by various combinations of capsule (K) loci. Coloured lines indicate the coverage by sub-continental region and globally. The left panel shows the coverage for combinations of K loci selected as the top 20 globally. The right panel shows the coverage for combinations of K loci selected as the top 8 from each region (some are overlapping). The target population coverage of 70% is indicated by the dashed line. The target is exceeded in all regions with the K locus combination on the right, but not that on the left.
Secondary vaccine targets, the O polysaccharides were much less diverse than the capsule polysaccharides, and our data showed that just 5 O types accounted for >86% of infections, but the potential efficacy of vaccines targeting these polysaccharides has been questioned.
So what does this mean?
Our work shows for the first time that it is theoretically possible to make a single multi-valent anti-capsule vaccine targeting >70% of infecting K. pneumoniae in all geographies, which is great news for vaccine design. Importantly, the data are an essential first step in prioritising capsule types for vaccine inclusion.
This was a huge collaborative effort including >80 contributors representing >70 organisations from 13 countries in Southern Asia and Africa, as well as Monash University (Australia), London School of Hygiene and Tropical Medicine (UK) and others. It was a privilege to work with such a diverse and knowledgeable team.
